
MRI (Magnetic Resonance Imaging) for Leiomyomas
Sebastian Harth Dr. med.
Universitatsklinikum, Giessen, Germany
Key Points
- Magnetic resonance imaging (MRI) is an important diagnostic tool used selectively in the evaluation of patients with leiomyomas
- The technique can be especially helpful in distinguishing adenomyomas from leiomyomas, for localization of tumors to assist the performance of abdominal myomectomy techniques, and to aid in the classification of the relationship between the leiomyoma and the serosa when evaluating individuals for hysteroscopic myomectomy.
- MRI is an integral aspect of one approach to targeting and guidance for high intensity focused ultrasound (HIFU).
Basics of Magnetic Resonance Imaging
Physics
Magnetic Resonance (MR) scanners use strong magnetic fields and radiofrequency (RF) energy to produce cross-sectional images. Clinical MR scanners utilize hydrogen protons for imaging. These are present in the human body in fat tissue and water and resemble tiny magnets, randomly aligned in the body in their normal state. The strong magnetic field in an MR scanner aligns the hydrogen protons. This is comparable to a compass whose needle is deflected when a magnet is held close. The alignment of the hydrogen protons leads to a net (longitudinal) magnetization. The protons also perform a rotational movement when placed in a strong magnetic field, like a spinning top exposed to gravity. This rotary motion is called precession, and its frequency is proportional to the field strength of the scanner. With the help of RF pulses at the precessional frequency of the protons, the protons can be deflected from their forced longitudinal orientation in the magnetic field. For example, a 90° RF pulse rotates the magnetization from the longitudinal into the transverse plane, leading to transverse magnetization. The RF pulse also leads to the precession of some protons in the same direction, i.e., “in phase”. Following an RF pulse, these protons send out signals that can be measured by coils. A computer calculates a series of cross-sectional images of the body from these signals using mathematical methods. By varying acquisition parameters such as the time between the emission of two RF pulses (repetition time) and the time from the emission of one RF pulse to the signal acquisition (echo time), pulse sequences with different image contrasts can be generated. The two main categories of pulse sequences are constituted by T1- and T2-weighted sequences (Pooley, 2005, Roth and Deshmukh, 2017).
T1
Following an RF pulse (e.g., 90°), the protons slowly realign in the longitudinal direction, determined by the strong magnetic field of the MR scanner. This is called T1 relaxation, longitudinal relaxation, or spin-lattice relaxation. Protons in different tissues vary in the rate the longitudinal relaxation occurs. By varying the repetition time, these differences can be used to acquire images that are T1-weighted or are not T1-weighted: A short repetition time can be used to generate T1-weighted images (tissues with short T1 appear bright, tissues with long T1 appear dark on images); a long repetition time can be used to generate non-T1-weighted images (imaging appearance of tissues is not dependent on T1). In T1-weighted images of the pelvis, fat, proteinaceous fluids, and certain breakdown products of hemoglobin (methemoglobin) appear hyperintense. Water (urine, cerebrospinal fluid), skeletal muscle, and the uterus appear hypointense (Hashemi et al., 2018).
T2
Following an RF pulse, the protons not only slowly realign in the longitudinal direction. Additionally, after a short time the precession of the protons does not longer occur in phase due to dephasing. This is called T2 relaxation, transverse relaxation, or spin-spin relaxation. The causes of spin dephasing are internal and external magnetic field inhomogeneities. By varying the echo time, differences in the rate of transverse relaxation in various tissues can be utilized to acquire T2-weighted images. A long echo time can be used to generate T2-weighted images (tissues with long T2 appear bright, tissues with short T2 appear dark on images); a short echo time can be used to generate non-T2-weighted images (image appearance of tissues not dependent on T2). In T2-weighted images of the pelvis, fat, free water (urine, cerebrospinal fluid), and bound water (e.g., in the endometrium and many inflammatory and malignant lesions) appear hyperintense. Skeletal muscle and the uterine junctional zone appear hypointense (Hashemi, et al., 2018).
Contrast-Enhanced Imaging
The ability to distinguish soft tissue is one of the main advantages of MRI. However, sometimes there is insufficient image contrast observed between different tissues, so the use of contrast agents is beneficial in various applications of MRI. Contrast agents with paramagnetic ion complexes containing gadolinium are most commonly used (gadolinium-based contrast agents, GBCAs). These lead to a shortening of the T1 and T2 times. Tissues that take up contrast media appear hyperintense in T1-weighted sequences and hypointense in T2-weighted sequences. Currently, GBCAs are mainly used for positive contrast in T1-weighted images, often with the use of fat suppression techniques. (Geraldes and Laurent, 2009, Xiao et al., 2016).
Diffusion-weighted imaging (DWI)
The utility of diffusion-weighted imaging (DWI) has been demonstrated primarily in oncologic imaging and in the visualization of inflammatory lesions. DWI utilizes the random motion of water molecules, commonly using a T2-weighted echo-planar sequence with dephasing and rephasing gradients. The signal of stationary protons is maintained by the effect of both gradients, while the signal of moving protons is suppressed (not experiencing both gradients and falling out of phase). As a result, hypercellular tissues rich in diffusion-inhibiting membranes exhibit a relatively higher signal (appearing hyperintense on DWI images). However, due to the inherent T2 hyperintensity (T2-shine-through), detection of true DWI hyperintensity as a result of diffusion restriction can be difficult. This problem is circumvented by generating images that represent the apparent diffusion coefficient (ADC-maps). ADC-maps are inverse diffusion-weighted, while DWI images are diffusion-weighted, but also considerably T2-weighted. Lesions that restrict diffusion (e.g., abscesses, malignant masses) increase the ADC and commonly appear dark on ADC-maps and bright on DWI images (Roth and Deshmukh, 2017). The main role of DWI and ADC in uterine imaging is to aid in the detection of rare leiomyosarcomas (Hindman et al., 2023).
Uterine Magnetic Resonance Imaging
Protocol Recommendations
Guidelines for MR imaging of leiomyomas have been published by the European Society of Urogenital Radiology (ESUR), including patient preparation, MRI technical considerations and reporting (Kubik-Huch et al., 2018). Following the ESUR-guideline, MRI examinations of the uterus for leiomyomas do not have to be planned according to the menstrual cycle. Fasting for 3-6 hours prior to the examination, emptying of the urinary bladder 1 hour before MRI and the use of antiperistaltic agents (20 mg butyl scopolamine im/iv or 1 mg glucagon iv) are recommended. The examination may be performed at 1.5 Tesla or 3 Tesla. The basic protocol comprises axial and sagittal T2-weighted sequences (option: oblique axial of the uterine corpus), and an axial T1-weighted sequence (option: T1-weighted sequence with fat-suppression, if high signal lesions are depicted). For indeterminate adnexal and uterine lesions (leiomyomas with atypical features, suspicion of malignancy), the addition of dynamic contrast-enhanced (DCE) sequences and, optionally, DWI is recommended. For pre- and post-embolization assessment, the addition of MR angiography or DCE sequences and DWI is advised.
The 2023 consensus statement by Hindman et al. on the evaluation of atypical uterine masses recommends performing the precontrast T1 sequence as an in- and out-of-phase sequence (Hindman, et al., 2023). Suggested slice thicknesses are 3 mm or less for the axial T2 sequence and the DCE sequence and 4 mm or less for the remaining sequences. most patients, the administration of GBCAs or other advanced imaging techniques will not be necessary to map leiomyomas. Nevertheless, the risk profile of GBCAs is regarded to be very good (Bashir and Thomas, 2023).
Rarely, severe hypersensitivity reactions are encountered. Direct clinical effects of gadolinium retention in the brain have not been detected so far. It is assumed that nephrogenic systemic fibrosis (NSF), a rare but clinically manifest disease caused by gadolinium deposits, occurs exclusively in patients with kidney disease. Still, contrast agents should only be used when necessary and non-contrast MRI techniques should be considered when appropriate. The use of GBCAs also incurs extra costs and time that can be avoided by performing examinations without contrast agents (Harth et al., 2023).
Normal Uterus
Figure 1 demonstrates the normal zonal anatomy of the uterus with T2-hyperintense endometrium, hypointense junctional zone and intermediate signal myometrium. A potential pitfall in MRI of the uterus are myometrial contractions, which are not to be confused with leiomyomas or adenomyosis (Figure 2).

MRI Appearance of Leiomyomas
Leiomyomas typically have well circumscribed margins and appear homogeneously hypointense on T2-weighted sequences and isointense or hypointense to normal myometrium on T1-weighted sequences (Raffone et al., 2024). In some cases, a high-intensity surrounding rim can be identified on T2-weighted images, corresponding to dilated lymphatic vessels, dilated veins, edema, or a combination of these features (Mittl et al., 1991). On contrast-enhanced MRI, although not necessary for diagnosis, leiomyomas show variable enhancement, often similar to the myometrium. On DWI, typical leiomyomas show low signal both on DW images and on ADC maps (T2-blackout).









Differential Diagnosis
Leiomyosarcoma
- Leiomyosarcoma typically presents as a new or enlarging solid uterine mass with irregular margins in postmenopausal women with moderate to high T2 signal intensity, high T1 signal intensity, and central non-enhancing areas (Raffone, et al., 2024).
- Features suggestive of sarcoma: Size, borders, DWI, hemorrhage, T2 dark areas, necrosis etc.
- Limitations to the specificity and sensitivity.
Adenomyosis
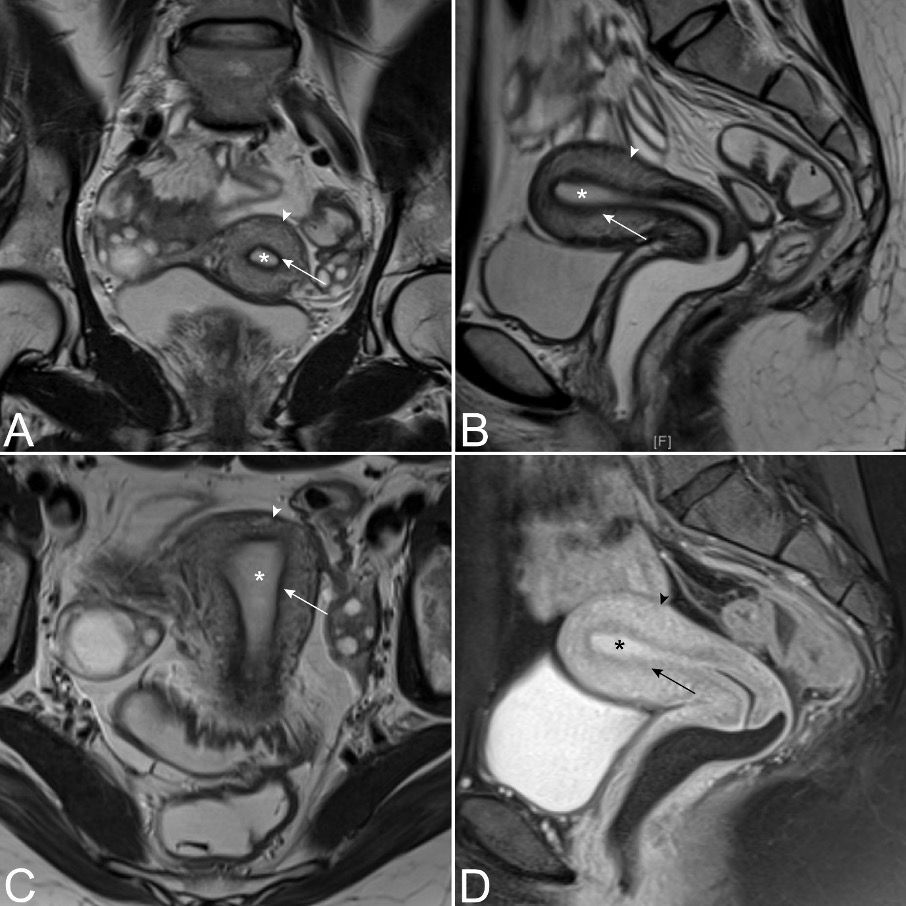
Adenomyosis is defined by the presence of endometrial glands and stroma located in the myometrium (Bird et al., 1972). The main subtypes of adenomyosis are internal adenomyosis, adenomyomas and external adenomyosis. Although the width of the junctional zone was originally thought to be a sign of internal adenomyosis, it could not be confirmed as a reliable criterion (Bazot and Darai, 2018, Tellum et al., 2019). The criteria with the highest specificity for diagnosing adenomyosis are considered to be an irregular appearance of the junctional zone, the presence of myometrial cysts, and adenomyoma (Tellum, et al., 2019) (Figure 20). In contrast to leiomyomas, adenomyomas are ill-defined myometrial lesions that commonly exhibit tiny cystic components or hemorrhagic components (Bazot and Darai, 2018) (Figure 21).
Conclusions
References