
Uterine Artery Embolization
Contributors: Mary Ann Lumsden MD, Esraa Algeria MD, James Spies MD
Key Points
- Uterine artery embolization (UAE) was the first image-guided technique for the management of bleeding and pressure symptoms related to uterine leiomyomas, and has robust evidence supporting its use as an alternative to hysterectomy.
- Appropriateness of the use of UAE in women with infertility or who wish to become pregnant in the future is unclear as there is less evidence relating to fertility and pregnancy performance, particularly that which is specific to the various leiomyoma phenotypes (FIGO Type, number, volume).
- Hysteroscopic myomectomy remains the most appropriate surgical intervention for those with FIGO Type 0, 1, and 2 tumors that can be removed safely using the intrauterine approach.
- UAE may have a role, even in women who wish further pregnancy, in specific instances where hysteroscopic myomectomy is not feasible, or when there exist risks to an abdominal approach to myomectomy because of comorbidities.
- The relative value of UAE compared to targeted leiomyoma ablative procedures such as microwave, radiofrequency, or focused ultrasound ablation remains unclear.
The incidence of leiomyoma increase as women enter their third and fourth decades. Also, in recent years, childbirth trends have shifted and more women appear to delay starting their families. Fibroids have a higher prevalence in African- American women signifying a marked disparity in health needs when compared with women of Caucasian origin (Stewart et al 2017: Etoukhi et al 2014) This trend may have driven an increased demand for uterine saving fibroid treatments (Fonseca et al 2017; Lessne et al 2019)). This change in demographics coupled with the increased availability of newer treatment options warrant that we should be able to advise patients on best evidence based treatment for them. More on the epidemiology and the pathogenesis of uterine fibroids and their symptoms is found elsewhere in this site.
The Procedure
Uterine artery embolization (UAE) is an interventional radiologic procedure that involves temporary occlusion of the uterine arteries using biocompatible particles. In most instances, UAE is performed under moderate sedation and local anesthetic. After accessing the right femoral artery, a radiopaque catheter is guided to one of the uterine arteries under fluoroscopic direction. After injecting the particles into the artery to the point of occlusion, the catheter is repositioned in the opposite uterine artery, where the process is repeated. This bilateral uterine artery occlusion results in ischemia from which the uterus recovers, but the fibroids do not, resulting in their infarction.
First described by Ravina from France in 1995 (Ravina 1995), UAE has since been demonstrated to generally provide sustained relief of leiomyoma-associated symptoms, most notably pressure and abnormal uterine bleeding (AUB). It has similar rates of patient satisfaction to myomectomy and hysterectomy (Cochrane ?, Others?). The procedure has also been reported from low- and middle-income regions in Africa and Asia, with reports of success even with large fibroids as are common in Africa. There are several reports of good outcomes, and overall, its introduction has been a positive experience for many women in both Africa and Asia (Mariara et al. 2017; Mutai et al. 2015; Subrmaniam et al. 2010)
While UAE has been demonstrated to be an effective, uterine-sparing alternative to hysterectomy, its role as an alternative to abdominal approaches to myomectomy, either laparoscopic or laparotomic, or other image-guided leiomyoma ablation techniques is less clear. Uterine artery embolization should not be seen as an alternative to hysteroscopic myomectomy when removal of types 0, 1, and 2 tumors is feasible.
ce itSee what you think-


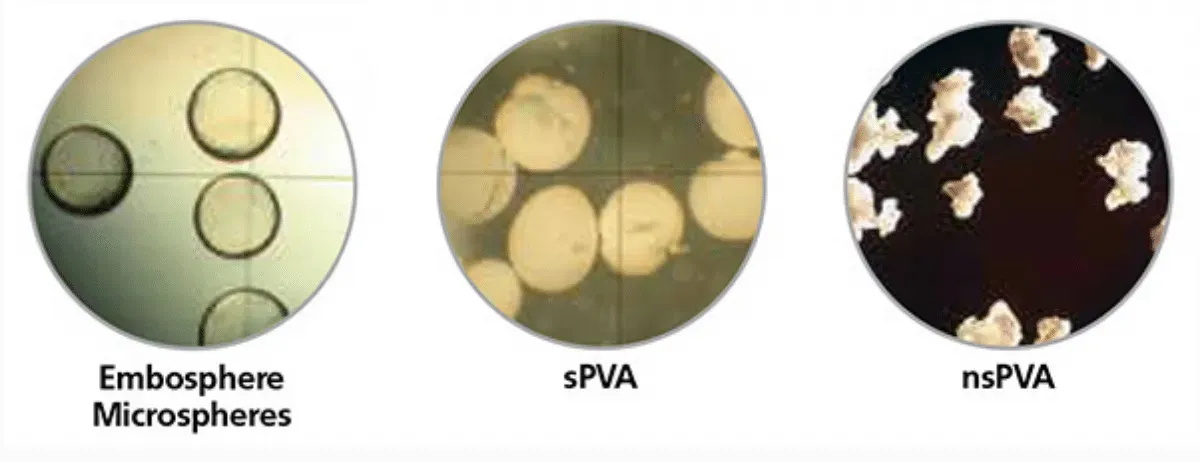
Embolic Agents
Permanent Material
- Polyvinyl alcohol particles
- Hydrogel microspheres
- Tris-acryl gelatin microspheres
Biodegradable Material
- Gelatin sponge particles or beads
- Calcium Alginate Gel
Clinical Outcomes
Summary
Following occlusion of the uterine arteries by embolization, fibroid infarction generally occurs with subsequent shrinkage and symptom resolution for most women. It is suspected that the molecular expressions associated with leiomyomas, such as TGF-𝛽3, described in the pathogenesis section (LINK), are also diminished or eliminated, but data supporting this hypothesis are unavailable. The expected outcomes following a UAE include a mean 50 to 60% fibroid size reduction, [MM1] 40 to 50% reduction in uterine volume, 88 to 92% reduction of bulk symptoms, greater than 90% elimination of abnormal uterine bleeding, and 80 to 90% patient satisfaction (Stewart et al. 2015) When compared with the abdominal approaches to myomectomy, UAE appears to improve the quality of life of women with symptomatic uterine fibroids to a similar degree (Need appropriate citation).
Given the similar outcomes from laparotomic or laparoscopic myomectomy and embolization, the choice of therapy should be based on patient preferences, patient-specific factors, and the availability of appropriately skilled providers. For those with infertility or who wish for future fertility, the issue is somewhat more complex as the comparative impact of UAE and laparoscopic or laparotomic myomectomy on fertility and subsequent pregnancy is not clear.
The lack of clarity regarding the impact of UAE on fertility is related to the fact that the randomized studies published to date have been plagued by small sample sizes and differing results. There had been concerns about the impact of UAE on ovarian function based on earlier studies of women who had undergone the procedure in their later forties (Reference?), However, randomized trials in younger patients have not demonstrated a diminution of ovarian reserve (Mara 2008, Sirkeci 2023). There are fewer data available on uterine function after UAE, and this suggests caution is warranted in recommending UAE to those seeking to become pregnant. While pregnancy can regularly occur after UAE, myomectomy may have better outcomes (Mara 2008). However, the data are weak and further study is needed, particularly comparing leiomyoma phenotypes such as number, volume, and location with respect to the myometrium and other features defined by the
FIGO leiomyoma classification system (Link).
Quality of Life
UAE provides substantial improvement in quality of life (QoL) measures after treatment. While myomectomy has a slight advantage statistically in QoL scores measured, from a clinical perspective, both QoL and symptoms are similar at two years (Manyonda et al. 2020).
Menstrual Blood Loss
Menstrual blood loss can be measured using a Pictorial Blood loss Assessment Chart
(PBAC) and UAE generally leads to a significant decrease. (Sirkeci et al 2023). Compared with myomectomy, there is no apparent difference in menstrual regularity with regular or relatively regular cycles in 88% of the UAE group and 61% of the myomectomy group, and the difference was not statistically significant (Which citation?). There are also no differences in the bleeding scores nor the proportions of women reporting amenorrhea or heavy bleeding; median PBAC scores decreased from 133 (IQR 63-275) to 32 (0-88) at two years in the UAE group and from 180 (100-383) to 41 (11-84) in the myomectomy group (Citation).
Fertility and Pregnancy outcomes
There is considerable uncertainty as to the impact of UAE on pregnancy (Gupta et al. 2014). Many studies have not included women wishing to become pregnant, and the recording of pregnancy outcomes has been variable since many women included have not actually wanted to become pregnant. Studies of [MM2] reproductive outcomes in women desiring pregnancy following UAE for symptomatic fibroids suggest an overall mean pregnancy rate of 39.4%, a live birth rate of 69.2%, and a miscarriage rate of 22%. ( Fertil Steril. 2014; fertnstert.2013[MM3] .)
The major confounding factor in most studies has been patient age, with most including women over 40 years who already have lower fertility compared to younger cohorts[MAL4] . Studies have often compared outcomes in women following UAE with those of the general population of women rather than age-matched women who also have fibroids. The miscarriage and pregnancy rates in the studies analyzed appear comparable to the age-matched population.
Because the data from rigorous studies assessing the impact of UAE on fertility are limited at this time, myomectomy is considered to be a better option for women who have Type 0 or Type 1 fibroids[MAL5] [MAL6] [MAL7] . Also, there are women who are not good surgical candidates, those with prior myomectomy, and others for whom myomectomy may be a good option but who choose a non-operative approach after appropriate counseling where UAE will be the first line treatment. (Torre et al 2014; Serres-Cousie et al 2021; Zanoli et al 2022).
Ovarian Reserve
This can be measured by assay of Follicle Stimulating Hormone (FSH), Anti-Müllerian
Hormone and Luteinising Hormone (LH). In a single study assessing women at one year following UAE, there was no adverse impact on markers of ovarian reserve, which was similar to the results following myomectomy (Sirkeci et al. 2023)
Re-Intervention Rate
At three years of follow-up, the overall re-intervention rate among patients who underwent UAE was 14.4%. [MM1] This is in keeping with multiple prior studies that concluded that UAE has a similar patient satisfaction rate compared to the other surgical alternatives and is associated with a shorter hospital stay[MM2] . For example, available data from China suggest that when comparing myomectomy and UAE, the frequency of repeat interventions was similar and, at five years, an equal proportion of women would recommend their procedure (Jun et al. 2020). Consequently, all women, including those desiring a future pregnancy, should have UAE discussed with them and, if appropriate, offered as an alternative to operative management.
Complication Rates
The overall complication rate after UAE differs from the published report and can be as high as 40% to as low as 5%. Much of this difference is due to varying definitions of adverse events, post-procedure pain management, and experience in treating patients. With appropriate post-procedure protocols, complications leading to re-admission post-procedure are well less than 5% (Worthington-Kirsch 2005) above.
Table: UAE Adverse Outcomes
The overall complication rate differs by published report and can be as high as 40% to as low as 5%.
| Adverse Outcome | Clinical Comment |
|---|---|
| Pelvic pain | Common, starting 10–20 min after completed uterine artery embolization and usually only lasting a few hours |
| Need for surgery | Rare (less than 1/100) |
| Vaginal discharge | Common initially (58%), usually self limited. |
| Abscess/other severe intrauterine infection | Rare (less than 1 in 100) |
| Post embolization syndrome | This flu-like illness occurs within 24-48 hours of the procedure and resolves within two days but may last up to seven days |
Patient Selection
UAE is appropriate for most patients with uterine fibroid symptoms, including abnormal and heavy bleeding, pain during sex, pelvic pain and pressure, constipation, urinary issues, and erratic menstrual cycles. UAE may be a preferred choice over surgery in the following circumstances:
- Ideal CandidatesI
- Patient wishes to avoid surgery, although they must be willing to accept hysterectomy in the event of an emergency (in 100)[MM1]
- Women who want to retain their uterus
- The patient wants to minimize time away from work and family.
- Patient who is not a good surgical candidate (obesity, bleeding disorders, anemia, refusal of blood products, prior pelvic surgery, etc.)
Contraindications
- Viable active pregnancy
- Malignancy of the uterus/cervix without concurrent surgical treatment planned
- Active endometritis
- Postmenopausal patient with bleeding of undiagnosed etiology
Relative Contraindications or Special Care Considerations
For patients with a severe allergy to iodinated contrast used in arteriography, appropriate prophylaxis with corticosteroids is indicated. Similarly, where there is a history of vascular surgery or vascular injury in the pelvis, caution with vascular access and embolization is needed.
There are certain fibroid types or locations that may not respond as well to embolization and therefore, surgery can be a better option. For example, small intra-cavity fibroids are usually better treated with hysteroscopic resection and very large sub-serosal fibroids can have a better outcome with myomectomy. Cervical fibroids are more difficult to treat with embolization, but in a woman where uterine retention is important, it may be a better choice than myomectomy. For women with very large fibroid uteri (those with a greater than a 24-28 week size or greater) may not have sufficient shrinkage after UAE to return abdominal girth to normal and those women, may prefer surgery.
There are specific circumstances when surgical resection has been planned but due to the size and/or number of fibroids, excessive blood loss is a concern. In this setting, pre-operative UAE followed by surgery can dramatically reduce blood loss and facilitate surgery.
References
Eltoukhi HM, Mode MG, Weston M, Armstrong AY, Stewart EA. The health disparities of uterine fibroid tumors for African American women: A public health issue. Am J Obstet Gynecol 2014; 210: 194-9.
Fonseca MCM, Castro R, Machado M, Conte T, Girao MJBC. Uterine artery embolization and surgical methods for the treatment of symptomatic uterine leiomyomas: a systematic review and meta-analysis followed by indirect treatment comparison. Clin Ther 2017;39:1438-55.
Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptoms uterine fibroids. Cochrane Database Syst Rev 2014;12:CD005073
Jun F, Yamin L, Xinli X, Zhe L, Min Z, Bo Z et al. Uterine artery embolization versus surgery for symptomatic uterine fibroids: a randomized controlled trial and a meta-analysis of the literature. Arch Gynecologist Obstetrics 2012;285:1407-13
Mantonda I, Belli A, Lumsden MA, Moss J, McKinnon W, Middleton L, et al. Uterine artery embolization or myomectomy for uterine fibroids. New Engl J Med 2020;383:440-51
Mariara C, Obura T, Hacking N and Stones W. One year symptom severity and health‑related quality of life changes among Black African patients undergoing uterine fibroid embolization. BMC Res Notes (2017) 10:240
Mutai JK, Vinayak S, Stones, Hacking N, Mariara C. Uterine Fibroid Embolization for Symptomatic Fibroids: Study at a Teaching Hospital in Kenya. Journal of Clinical Imaging Science Vol. 5: Jan-Mar 2015
Subramaniam RN, Vijayananthan A, Omar SZ, Noor Azmi MA, Nawawi O, Abdullah BJJ, Uterine artery embolisation for symptomatic fibroids: the University of Malaya Medical Centre experience, Biomed Imaging Interv J 2010; 6(3):e27
Next Citation